“I felt what was being done was very close to … an institutional form of murder…it had become an accepted thing within the Public Health Service…not subject to review.” —Peter Buxtun, Tuskegee Syphilis Study whistleblower.
Such is the case with Lyme disease.
If it wasn’t bad enough that the long-term health complications can be utterly disabling, Lyme causes the literal destruction of lives, the disintegration of families and friendships, the sanctioned dogpile of mockery and abuse of sick people, the intentional withholding of care and benefits by our public health agencies.
Go for a walk in the park, get a tick bite, and BOOM, your life as you knew it is over.
Lyme disease is a disease that has been politicized like no other. If it makes the news, usually the story devolves into the “controversy” over whether “chronic Lyme” exists. Then it leads into the issue of the failed vaccine, LYMErix. Media laments the fact that there currently is no vaccine to prevent the horror and devastation wrought by this chronic disease that, as far as government health agencies are concerned, doesn’t officially exist. At the same time they downplay the extent of the problem, they claim we need a vaccine to combat it.
Tick bite victims are subjected to ongoing sociopolitical violence and denial of care because the “authorities” are throwing an epic tantrum. They wanted their vaccine on the market purely to make money and to create the illusion that the problem was being handled. We’re called anti-science, anti-vaccine, fakers, frauds, and much, much worse, by the very people who employed that strategy.
The implication is that those of us who already have suffered for years—decades, even—are turding up our own punch bowl by seeking to understand why we are so sick and why nobody believes us. In that process we inevitably expose some facts that those “authorities” would prefer stay buried. We expose criminal acts that include scientific research fraud, racketeering, medical malpractice, “color of law” abuses, and potentially homicide—an “institutional form of murder”—a charge based on the enforcement of policy that dictates this disease go undiagnosed and untreated.
Tell me: is there a vaccine for syphilis, another spirochetal disease whose devastating effects are frequently compared to Lyme? No. Spirochetal diseases have long been known to cause a permanent brain infection and immune suppression that can’t be vaccinated against. Syphilis was acknowledged to be such a terrible disease that it warranted a secret four-decade-long “study” in which the U.S. Public Health Service (now known as the CDC) committed atrocious human rights crimes against unwitting participants.
People of Color were exploited by the Public Health Service to study the dementia of tertiary syphilis under the guise of free health care and burial. The study notoriously withheld diagnosis and treatment so the disease progression could be observed until the victims died. Then the CDC and Johns Hopkins University repeated the experiment in Guatemala. All that carnage, and it never produced a vaccine.
More than 40 years into the tragedy of Lyme disease, those of us whose lives have been destroyed by it ask ourselves, “Is this another Tuskegee?” By all accounts, yes. Diagnosis withheld. Treatment withheld. Victims slandered. It is an institutional form of murder. An accepted thing…not subject to review.
How did we get here? How did we get to a place where you cannot walk into a doctor’s office, say the word, “Lyme,” and expect to walk out with a shred of credibility or dignity intact, let alone some relief from the unrelenting symptoms? How did we get to a place where family and friends believe those doctors and will turn their back on you for being “overly dramatic”? How did we get to a place where disabled, bedridden people have to do their own activism, fighting for their lives? A place where vile, denialist MDs openly bash such activists in the media and on platforms like Twitter? Where children are sentenced to a life of pain and disability? Where people are denied disability benefits and are left homeless? This place is Hell on earth, and this is how we got here:
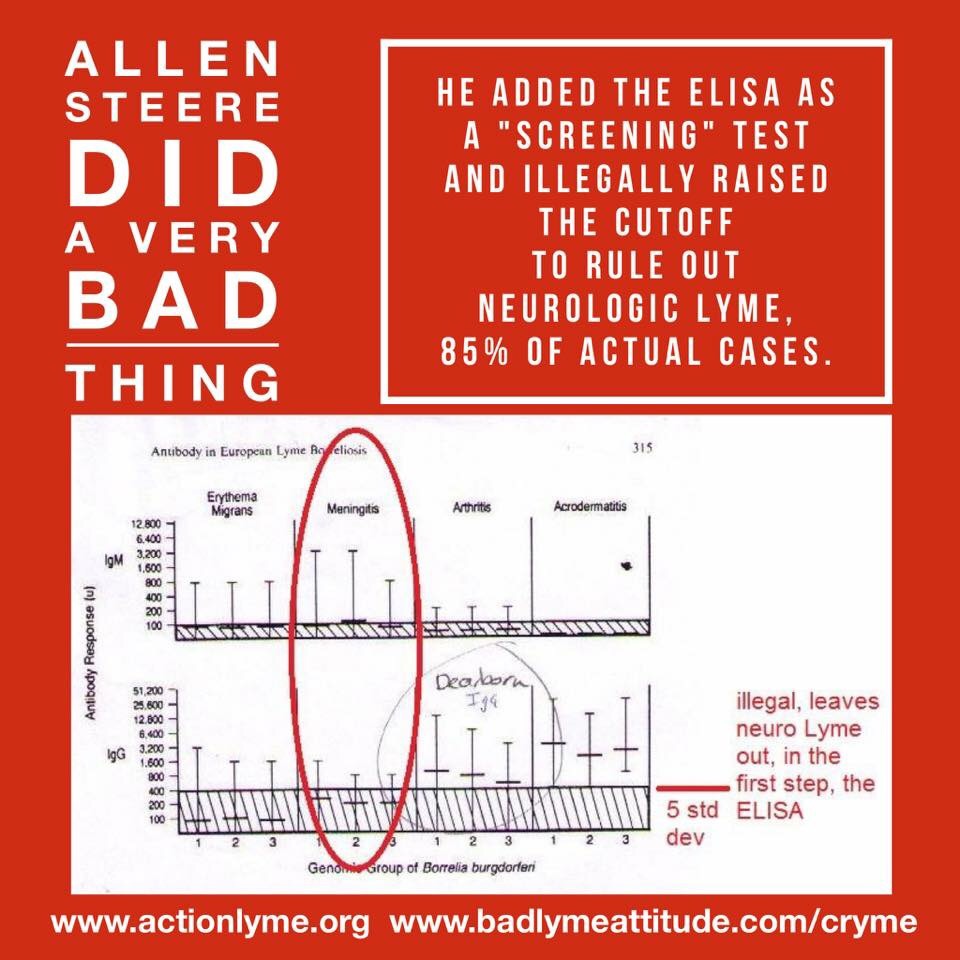
It is clear that even before the disease had a name, Allen Steere, who is commonly credited as being the co-discoverer with Willy Burgdorfer of “Borrelia Burgdorferi”, or Lyme disease, knew that most people did not mount a vigorous immune response. In a 1980 letter from Burgdorfer’s archives, Steere states, “Control patients generally had titers like those seen in case patients.”
Steere later said about seronegative Lyme disease, “I am convinced this entity exists.”
Throughout the 1980s he published reports about “fetal demise” from congenital infection, chronic neurologic symptoms in patients he followed for years, and the similarities to cancer.
Stephen Malawista, who worked alongside Steere when they were both at Yale in the very early days of Lyme discovery, was quoted in his obituary in the New York Times:
“What is the immune system if not a guard dog?” Why has it stopped responding to the spirochetes in its midst?”
Another fellow Yale researcher, Army and National Cancer Institute pathologist Paul Duray also noted similarities between Lyme and cancer. He said in 1989, “Immature B cells can be seen in the spinal fluid. These cells can appear quite atypical—not unlike those of transformed or neoplastic lymphocytes.”
(Duray, PH. Clinical pathologic correlations of Lyme disease. Rev Infect Dis. 1989 Sep-Oct;11 Suppl 6:S1487-93. PMID: 2814170)
In 1988, Raymond Dattwyler, Benjamin Luft, John Halperin, Marc Golightly and David Volkman at SUNY-Stony Brook published a report titled “Seronegative Lyme Disease,” in which they stated,
“We studied 17 patients who had presented with acute Lyme disease and received prompt treatment with oral antibiotics, but in whom chronic Lyme disease subsequently developed. Although these patients had clinically active disease, none had diagnostic levels of antibodies to B. burgdorferi on either a standard enzyme-linked immunosorbent assay or immunofluorescence assay. On Western blot analysis, the level of immunoglobulin reactivity against B. burgdorferi in serum from these patients was no greater than that in serum from normal controls.”
http://www.nejm.org/doi/full/10.1056/NEJM198812013192203
They also noted a dissociation between T and B cell responses, with a blunted B cell response, which led them to develop a T cell assay for diagnosis of “seronegative” cases. Allen Steere later used this “seronegative Lyme assay” in his own research.
The next year the same group reported that treatment fails in half of cases.
And what does it look like when treatment fails, or when diagnosis altogether is denied and no treatment is given?
“Not only are plasma cells plentiful in the spleen, lymph nodes and bone marrow, they are also represented by large and somewhat atypical-appearing precursor B cells as well.
“Numerous names have been given to this stage, including pseudolymphoma, lymphoid hyperplasia, follicular hyperplasia, lymphocytoma cutis, Spiegler-Fendt lymphoid hyperplasia, and lymphadenosis benigna cutis of Baverstedt.
“The immune response involves virtually all of the organs and structures of the reticuloendothelial system including the bone marrow, and clinical pain and discomfort seems to correlate with hyperplasia of lymph nodes and spleen and bone marrow. Diffuse visceral involvement in this acute stage mimics infectious mononucleosis or disseminated viral syndromes. These include conjuctivitis, pharyngitis, pneumonitis with dry cough and mild pleuritic pain, hepato-splenic tenderness, lymph node swelling of the neck and groin, and orchitis. There is lymphoid hyperplasia of the lymph nodes and spleen consisting of prominent germinal centers and numerous perifollicular lymphocytes, with proliferation of plasma cell precursors and mature plasma cells. The plasma cell precursors are large, appear tumor-like, and can resemble Reed-Sternberg cells.”
Alan Barbour, former colleague of Willy Burgdorfer at Rocky Mountain Labs, in 1988:
“The second-stage neurologic disorders may appear suddenly a few weeks after appearance of ECM or advance insidiously over months (82, 84,129,142, 145, 168). Approx- imately 30 to 40% of patients with disease progressing beyond ECM have neurologic complaints. In the early stages there may be clinical and laboratory evidence of meningeal iritation; in endemic areas B. burgdorferi is a common etiology of “aseptic meningitis.” Later a meningoradiculopathy with a lymphocytic pleocytosis and oligoclonal peaks in the cerebrospinal fluid(CSF) may come to the fore; this constellation has been termed lymphocytic meningoradiculitis or Bannwarth’s syndrome (82,84,145). Patients typically complain of headache and sharp pains in the trunk or extremities; there may be sensory and motor deficits as well. Unilateral or bilateral Bell’s palsy is often present, either by itself or associated with the radiculopathy. Some patients with chronic meningitis complain only of headache and extreme fatigue. During second-stage neurologic disease there may be evidence of encephalitis with altered mental status and diffuse slowing on the electroencephalogram. In the third stage of the disease, years after onset of infection, patients may present with such signs of diffuse or local cortical involvement as intellectual deterioration, hemiparesis, or unaccountable psychiatric abnormalities (3).
“The organism, like other pathogenic spirochetes, is prob- ably transmissible via the placenta to the fetus (17). B. burgdorferi infection of fetuses has been documented (114, 146).”
Imagine this all happening at the same time we were faced with the terror of the AIDS epidemic. By 1989 Lyme was known to be a chronic, neurologic disease of immunosuppression for which antibiotic treatment failed in half the cases. It was spreading quickly across the Northeast, upper Midwest and West Coast. It was reported in the media that SmithKline was was performing 2,500 Lyme tests per day at its Philadelphia lab.

Patients were already organizing support and advocacy groups. Infusion companies were popping up all over the Northeast to provide intravenous antibiotics, the standard treatment at the time for neurologic Lyme. The insurance companies were freaking out about paying for IV antibiotics for the entire East Coast–let alone the rest of the country–at the rate Lyme was spreading. From the perspective of the CDC, public health authorities and insurance industry, the situation was like a mob hit gone wrong. They needed to send in the cleaners and control the situation.
Enter the American Lyme Disease Foundation
In another piece of correspondence from the Burgdorfer archives, Leonard Sigal of Yale and later Robert Wood Johnson Medical School, implored his fellow researchers to organize AGAINST patients. Citing hysteria in the public and the media, he stated,
“It has become apparent that we, the scientific and medical community must do a better job of educating the public. We have absented our responsibility in this area and this vacuum has been filled by other organizations, less rigorous in their examination of ‘facts”. Unsupported speculation has been presented as truth, apprehension has replaced appropriate concern in endemic communities. The hysteria and medical malpractice associated with Lyme disease is actually obscuring the true severity of the public health problem. It is time that the scientists, physicians, and educators who work with Lyme disease organize to respond to these problems.
“This long letter is my first attempt to organize us into an effective counterforce to the various purveyors of misinformation and hysteria….It is our responsibility to respond to ignorance, quackery, and personal attack in a responsible fashion. By organizing and making ourselves available we can diminish the pathologic influences which are currently the sole source of public and media information on Lyme disease. We have not been active in this arena thus far in the history of the Lyme disease public health problem. Events are accelerating so that a response by a united front is needed now. I very much hope that you will join me in this effort.”
The American Lyme Disease Foundation (ALDF) was formed shortly thereafter to fulfill the public relations needs of a larger coalition of government officials and academic researchers whose goals were evident. They sought to obscure, through victim-blaming and slanderous journal reports, an epidemic that had emerged in parallel with HIV/AIDS, while also exploiting their ability to profit through total control of the dialogue.
Congress had recently passed several laws that opened the doors wide for those profit motives.
- 1980: The Bayh-Dole Act allowed individuals, universities and corporations to profit (via patents) off of research done on the government dime.
- 1980: The Stevenson-Wydler Technology Innovation Act literally required federal laboratories to participate in commercialization of their patents with outside corporations.
- 1986: The Federal Technology Transfer Act amended the Stevenson-Wydler Technology Innovation Act of 1980 to establish cooperative research and development agreements, or CRADA. A CRADA is a partnership between a government agency and outside organizations that provides numerous incentives and protections to all involved parties. Notably, it allows them to keep research results confidential for up to five years under the Freedom of Information Act.
- 1986: The National Childhood Vaccine Injury Act (NCVIA) diverted liability from pharmaceutical companies for injuries sustained from childhood vaccines, including vaccines that were being commercialized under CRADAs with the CDC or other federal agencies.
With Lyme, the trick would be first to “standardize” the testing, and then to market a vaccine. The testing strategy would give the CDC control over the diagnostic devices used, as well as the interpretation of results. The vaccine strategy would provide the public a sedative effect, calming the “hysteria” over this heretofore-incurable immunosuppression disease.
What ended up happening is that they rigged the testing so the “seronegative” cases were no longer a part of the disease definition, and then put out a vaccine that was made with a part of the bug that actually causes the disease. By throwing out the majority of cases which were seronegative, the Lyme profiteers could say that the adverse events that looked exactly like the disease manifestations were purely coincidental.
Benjamin Luft of SUNY-Stony Brook said it at the 1998 FDA meeting where Lyme vaccine development was the topic of discussion.
http://www.fda.gov/ohrms/dockets/ac/98/transcpt/3422t1.rtf
“The point that I wanted to make in regard to the study is that there is very heavy dependence on serologic confirmation. And when we start thinking about the adverse events, it was stated originally when we got the overview of the disease that the disease is really quite protean. And actually the adverse events are very similar to what the disease manifestations are.”
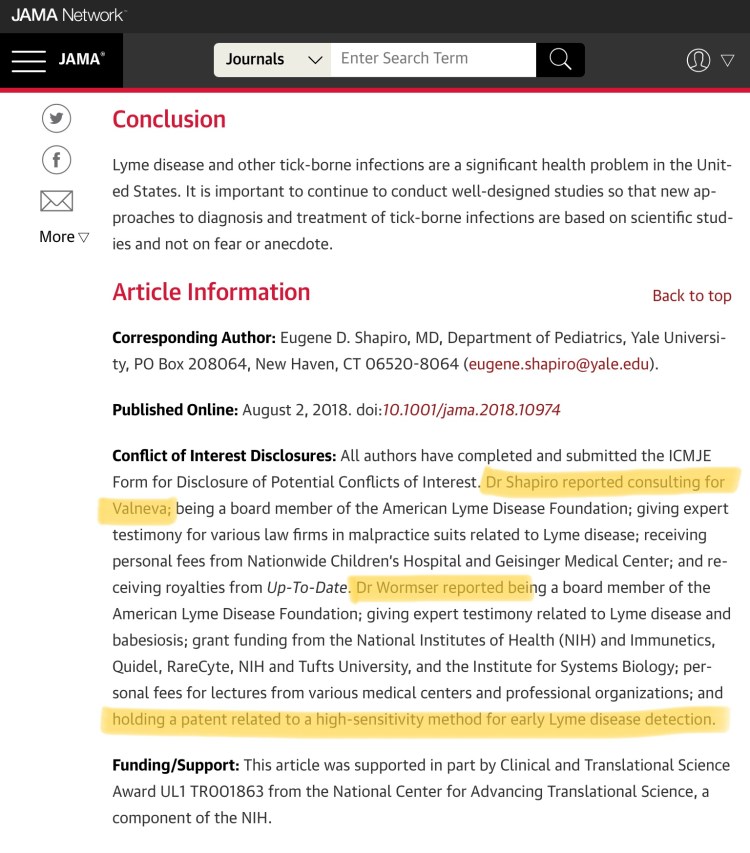
Dave Persing of the Mayo Clinic and Yale’s Robert Schoen developed and patented a diagnostic test in 1994. They echoed Luft’s sentiment in their patent application.
“Additional uncertainty may arise if the vaccines are not completely protective; vaccinated patients with multisystem complaints characteristic of later presentations of Lyme disease may be difficult to distinguish from patients with vaccine failure….”
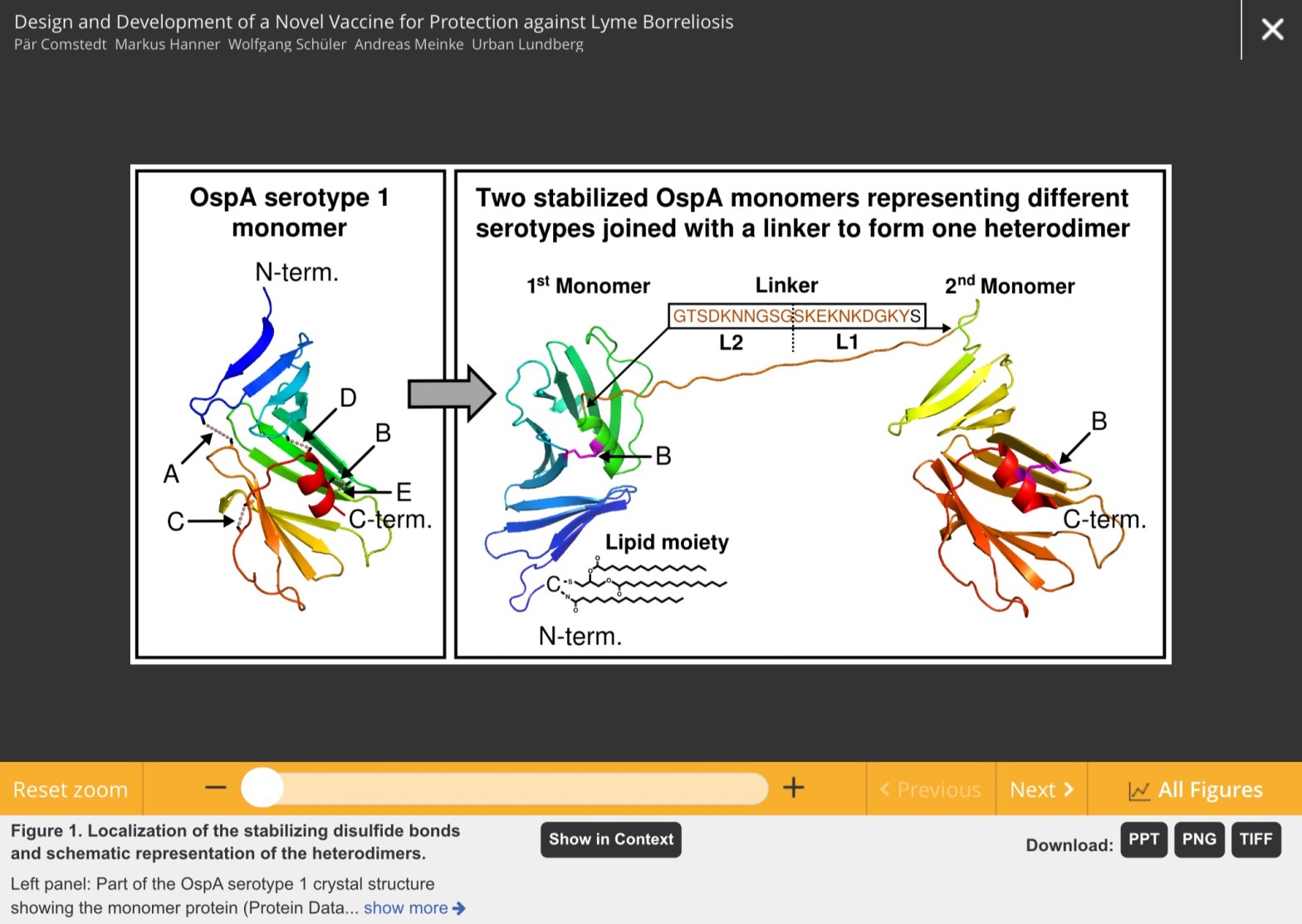
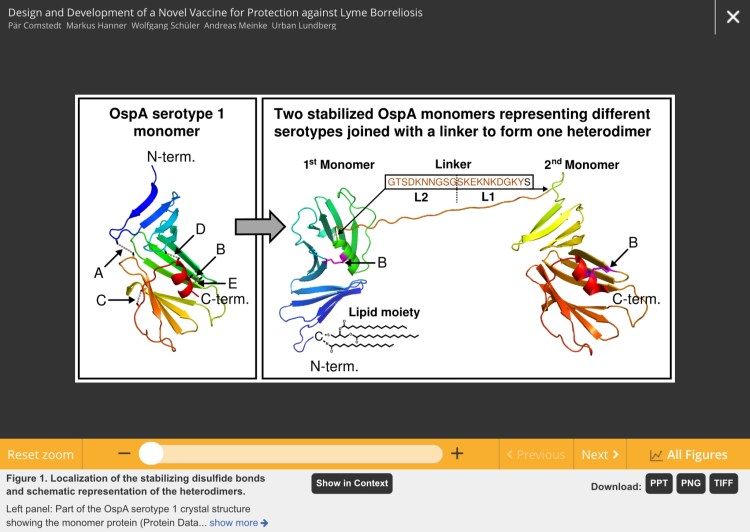
In fact, it was known early in Lyme vaccine trials that a specific part of the antigen used–the lipid part of Outer Surface Protein A (OspA)–is what caused the immune response, and therefore, also caused the adverse events which looked “very similar to what the disease manifestations are”.
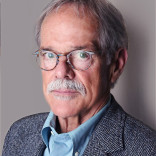
Alan Barbour, who patented OspA and stood to profit from any and all of its commercialization, worked with Pasteur Merieux Connaught in the development of their OspA-Lyme vaccine. Barbour and Connaught published in 1993 that OspA was not immunogenic without the lipids attached. In other words, it’s the lipids that cause the disease, whether delivered by OspA in a vaccine preparation or OspA on a spirochete. In a flagrant conflict of interest, Barbour also served on the Data & Safety Monitoring Board for the Connaught vaccine trials, knowing full well that OspA was the opposite of a vaccine.
Raymond Dattwyler and the SUNY-Stony Brook group also had found the lipids to be problematic. In 1988 they reported that the “supernatants”, or these borrelial lipids, are responsible for inhibiting natural killer cell activity. The lipids are present on most of the Osps–not just OspA–according to Mario Philipp, a prominent Lyme researcher from Tulane University.
Allen Steere was the lead investigator for the SmithKline LYMErix vaccine trials. SmithKline was tapped by Yale to commercialize its vaccine patent, and had a CRADA with the CDC to do so. Steere was at the June 1994 FDA meeting where Raymond Dattwyler told the FDA Vaccine Committee that the patients with low or no antibodies are the sickest:
“– the ones that failed to mount a vigorous immune response tended to do worse. So, there is an inverse correlation between the degree of serologic response and the outcome.
“So, individuals with a poor immune response tend to have worse disease.”
Follow:
If the lipids of OspA cause “Lyme disease” of both the arthritic knee (high antibody) and immunosuppressive (low antibody) varieties–regardless of whether they are injected by tick or syringe;
And the disease’s case definition includes both outcomes;
Then trials for a “vaccine” that’s made of lipidated Ospa cannot be deemed successful unless the sickest cases are excluded from the definition.
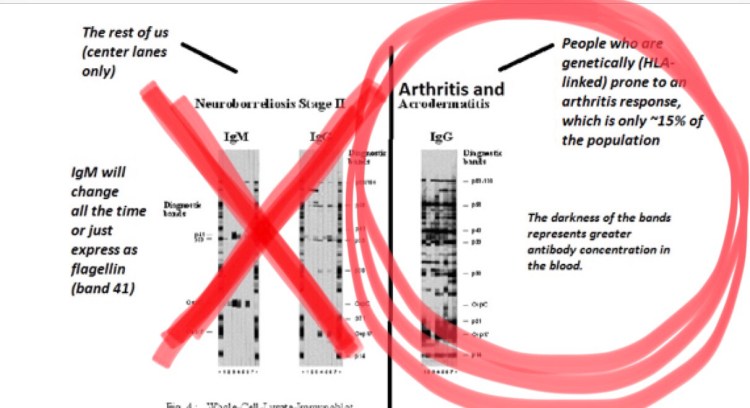
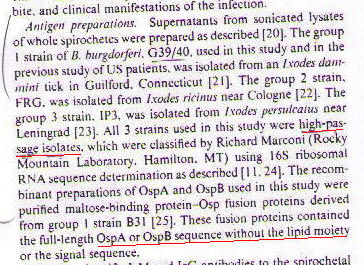
The Lyme mafiosos knew they had to falsify the testing to qualify their fake vaccine. And all involved—Yale, Allen Steere, SmithKline and the CDC—knew that people with certain “human leukocyte antigens” or HLAs (genetic factors) tend to manifest a single arthritic knee with no other symptoms. Said Allen Steere in 1993:
“When single serum samples from 80 patients with Lyme arthritis, were tested, 57 (71%) showed antibody reactivity to recombinant Osp proteins; in contrast, none of 43 patients who had erythema migrans or Lyme meningitis (P < 0.00001) and 1 of 5 patients who had chronic neuroborreliosis but who never had arthritis (P = 0.03) showed antibody reactivity to these proteins.”
Late Lyme arthritis cases, known to have a single arthritic knee and no other symptoms, produced antibodies to the Osps. Chronic, neurologic meningitis cases did not. By limiting the disease definition to the high-antibody arthritis cases only, it could be claimed that LYMErix induced a strong (read: protective) immune response, and that the systemic adverse events identical to seronegative Lyme were completely unrelated.
It would require an institutional form of murder to get a Lyme vaccine on the market.
The Testing
In the late 1980s, when the Lyme situation was spinning out of control and the SmithKline lab was performing 2,500 tests every day, diagnostics were left up to private labs in an open market. There were labs all over the country who could carry out simple immunoassays and Western blots. Therefore, the key to ensuring that only the not-sick cases got diagnosed was controlling and centralizing the testing.
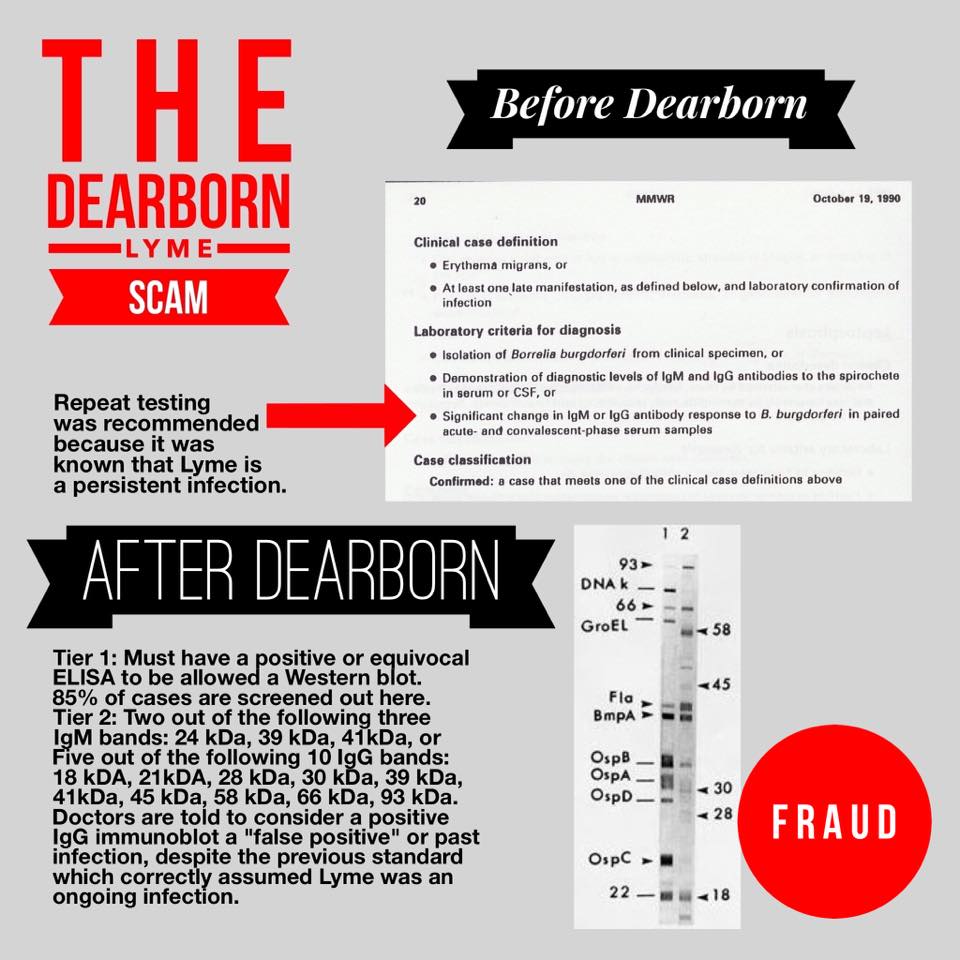
Discussions about “standardizing” the testing began in earnest in 1990, at the “First National Conference on the Serologic Testing of Lyme Disease”, and culminated in the falsification of the case definition at the Second National Conference in 1994. The CDC’s Barbara Johnson and David Dennis played ringleaders for these conferences, which brought together all the big names in Lyme disease. The 1994 conference has come to be known simply as “Dearborn”, for the city in Michigan in which it earned its infamy.
Dearborn was advertised as an opportunity for the various labs to weigh in on the proposed standardization. Little did they know, the outcome had been predetermined by a “working group” composed of CDC officers, ALDF members, individuals with patent interests, and members of the Association of State and Territorial Public Health Laboratory Directors (ASTPHLD).
In fact, the conference was held in Dearborn because the CDC had arranged for public health laboratories to take over all of the testing, and Robert Martin, the president-elect of the ASTPHLD was also the laboratory director for the Michigan Department of Health. ASTPHLD had a CRADA with CDC that may or may not have been related, and may or may not have constituted a kickback situation.
It turned out that only one lab–MarDx–agreed with the proposal, and they had been provided prequalified serum samples. The others, when using the proposed testing scheme, came up with an average 15% accuracy. They protested, but it didn’t matter. The issue was not “subject to review”.
Lyme disease testing was no longer an issue of scientific validity. Indeed, there are standards for validation of a scientific method, and the new testing scheme flew in the face of those standards. The testing became an issue of detecting the genetically competent producers of abundant antibodies–the opposite of the FDA requirement for “Limit of Detection”. This is the requirement that a test be able to detect the lowest possible concentration of the analyte in question—in this case, borrelia antibodies.
The FDA never approved the method, either in the New Drug Application for LYMErix (SmithKline would have been required to prove their trial diagnostics were valid.), or in legitimate applications to the FDA for diagnostic test kits. MarDx ended up putting its test kits on the market in early 1996 through the 510(k) approval process. They cited the Allen Steere/Frank Dressler interpretation of the Western blot test (a study included in the Dearborn proceedings booklet) as the “predicate device”, meaning, they lied to the FDA about their tests being “substantially equivalent” to another device already on the market.
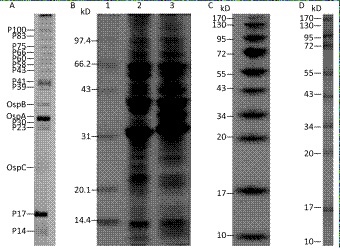
Regardless of the devices approved (or not) for testing, the critical issue is that of the interpretation of the tests. That is what the CDC dictates and controls through the ASTPHLD (now Association of Public Health Laboratories, ‘APHL’). Western blotting is a dinosaur in the world of diagnostics. It is a crude tool that measures the immune response to various antigens by the appearance of blots, or “bands” on a test strip. The more, and the darker, bands that appear, the stronger the immune response.
Whereas the prior standard for diagnosis simply called for a change in banding over sequential blots, the “Dearborn” standard required first a positive or equivocal result on an “ELISA” general antibody test, followed by the appearance of two out of three CDC-selected IgM bands and five out of 10 CDC-selected IgG bands on the Western blot. Obviously that in no way constitutes the lowest possible concentration of anything.
This is the institutional form of murder…accepted within the CDC and FDA…not subject to review…that has been excluding very ill people from diagnosis since 1994. Yes, this standard is still in place today. It is a form of torture, a human rights abuse, and a crime against humanity. And the people who committed this atrocity to this day have maintained their positions of authority and are still seen as the top experts in Lyme disease.
But the kicker remains the fact that LYMErix was pulled off the market after just three years because of the terrible adverse events that it caused. There were lawsuits, FDA hearings, a whistleblower; yet SmithKline was allowed to quietly withdraw its debacle of a vaccine supposedly due to low sales. If sales were lower than expected, one could reasonably conclude that word had gotten out that it was making people extraordinarily ill—disabled, even—with symptoms curiously mimicking Lyme disease itself.
Getting to Truth
It is understood within the Lyme patient community that the leading cause of death is suicide. The last quarter century has been a very dark time. But we are seeing glimmers of light.
There are scientists who have further explained the mechanisms of immunosuppression from OspA (its lipids) and the other Osps. Nicole Baumgarth of UC-Davis has described tolerance and cross tolerance (inability of the immune system to identify invaders) from Borreliae. Linden Hu of Tufts University recently was awarded a grant to study these mechanisms. Adriana Marques of the NIH described the disease as inducing humoral immunosuppression with chronic brain inflammation. A group funded by the Bay Area Lyme Foundation reported,
“The data show that patients who did not demonstrate strong B-cell immune responses were more likely to experience post-treatment symptoms….
“In addition to an association between plasmablasts and disease resolution, researchers also found that patients with persistent symptoms had a lower antibody response; more specifically, these patients exhibited reduced clonal expansion of B-cells.”
Most importantly, we know that OspA is a triacyl lipoprotein (as are, likely, the other Osps), and as such, it is a simple task to elucidate its effects on human health. Anyone can look up the research in the National Library of Medicine database, known as “PubMed”. In short, triacyl lipoproteins cause sepsis, and the preeminent researchers in the field of sepsis tell us that profound immunosuppression is a long-term complication of post-sepsis syndrome. See the publications of Richard Hotchkiss at Washington University in St. Louis–perhaps the top sepsis researcher in the United States.
Karen A. Cavassani and Steven L. Kunkel of the University of Michigan wrote in the journal BLOOD, JUNE 3, 2010:
“The post sepsis-induced expansion and enhanced function of regulatory T cells create an environment to potentiate tumor growth.
“It is becoming clear that compensatory anti-inflammatory response syndrome is actually a protracted immunosuppressive state in post septic patients, which may last for years. The immunoregulation in these patients is associated with both the inability to eradicate a primary infection and the development of new secondary infections. The question remains: why does “immunoparalysis” persist in the post septic immune system?”
A well known result of immunosuppression is the reactivation of herpesviruses.
A well known result of chronically active herpesviruses, particularly Epstein-Barr, is cancer.
“There is lymphoid hyperplasia of the lymph nodes and spleen consisting of prominent germinal centers and numerous perifollicular lymphocytes, with proliferation of plasma cell precursors and mature plasma cells. The plasma cell precursors are large, appear tumor-like, and can resemble Reed-Sternberg cells,” said Allen Steere.
“Immature B cells can be seen in the spinal fluid. These cells can appear quite atypical—not unlike those of transformed or neoplastic lymphocytes,” said Paul Duray.
We have cracked the code of the most politicized disease in the history of diseases. Lyme disease is really a form of tick bite sepsis, and what we know as “Chronic Lyme” is really post sepsis immune dysfunction, featuring immunosuppression, failure of antigen presentation, collapsed B cell germinal centers, tolerance and cross tolerance, fatigue-inducing herpesviruses and opportunistic infections of all kinds. But is this the end of the story? Not quite.
Remember the ALDF P.R. strategy to obscure and minimize Lyme disease? All these years they have redirected the seronegative cases toward diagnoses of fibromyalgia and chronic fatigue syndrome. They turned “Lyme disease” into a high-antibody arthritic knee, while the people who were really sick with seronegative disease were shuffled off to psychiatry or the next-most-politicized diagnosis–chronic fatigue. So, it looks like we’ve cracked that code, as well.
But wait…there’s more.
Dr. Jeffrey Fried, a Santa Barbara, CA internist, shed some light on the issue of post-sepsis in his 2016 article, “The Deafening Silence of a Spreading Sepsis Epidemic“. He wrote,
“A cancer survivor always knows they had cancer, but more often than not, survivors of sepsis have no idea they had sepsis. The media and the medical community have done a poor job of associating the term sepsis with these varied infections. Therefore, there is limited awareness of this disease, and there is no constituency to push for more funding for research into its nature and treatment.”
No constituency?
What if 30 million people in the U.S. were suffering from an incapacitating mystery illness that tore families apart and left people bankrupt or homeless? What if a million people a year were becoming disabled from a suspected bite of a disease-carrying tick, but could not get medical treatment or even acknowledgement that they were sick? What if a quarter of a million Gulf War veterans, and untold thousands more soldiers from subsequent wars, were being tortured by their own country through the whitewashing of their illness as “medically unexplained symptoms” (MUS)? What if all of these people were actually suffering from having no idea that they were survivors of sepsis, and that their chronic illness could be attributed to post-sepsis syndrome?
Because they are.
In the era of big data, there exists plenty of data to know what’s ailing 30 million U.S. citizens—considered medical mysteries—whose primary symptom is crippling fatigue. Surely there is enough empirical data for MDs to connect the dots for a tenth of the patients in their practice. The data is there, the cost to the “healthcare” system is in-your-face astronomical, one in every ten of our Facebook friends has a mystery illness, and yet, nobody seems to care. Not the CDC. Not the NIH. Not medical professionals on the front lines. There must be some reason that an “institutional form of murder” is “an accepted thing…not subject to review.”
Under the current regime, there is no outrage; there is no panic; there is no media coverage of the systematic disablement of a tenth of our population. Institutional forms of murder are just another day at the office for the power brokers of “healthcare”.
This is why we need to take the situation into our own hands and be the constituency that Dr. Fried says is nonexistent. We exist. They have tried to erase us, but we are here. We are the post-sepsis constituency–30 million and growing.
From the August 2018 article, As disease-bearing ticks head north, weak government response threatens public health, by Kristen Lombardi and Fatima Bhojani of the Center for Public Integrity:
“States where Lyme hardly existed 20 years ago are experiencing dramatic changes. In Minnesota, deer ticks and the illnesses they cause appeared in a few southeastern counties in the 1990s. But the tick has spread northward, bringing disease-causing bacteria with it. Now, in newly infested areas, says David Neitzel, of the Minnesota Department of Health’s vector-borne disease unit, “We haven’t been able to find any clean ticks. They’re all infected.”
“They’re all infected.”
Pretty soon they won’t merely be talking about the ticks.














You must be logged in to post a comment.